Source: http://www.aliem.com/paucis-verbis-card-abg-interpretation/
ABG Interpretation
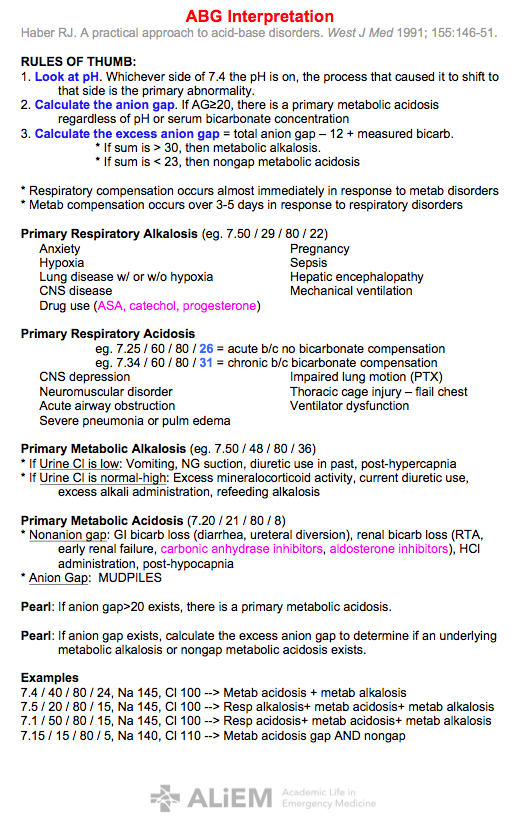
Haber RJ. A practical approach to acid-base disorders. West J Med 1991; 155:146-51.
RULES OF THUMB:
1. Look at pH. Whichever side of 7.4 the pH is on, the process that caused it to shift to that side is the primary abnormality.
2. Calculate the anion gap. If AG≥20, there is a primary metabolic acidosis regardless of pH or serum bicarbonate concentration
3. Calculate the excess anion gap = total anion gap – 12 + measured bicarb.
* If sum is > 30, then metabolic alkalosis.
* If sum is < 23, then nongap metabolic acidosis
* Respiratory compensation occurs almost immediately in response to metab disorders
* Metab compensation occurs over 3-5 days in response to respiratory disorders
Primary Respiratory Alkalosis (eg. 7.50 / 29 / 80 / 22)
Anxiety
Hypoxia
Lung disease w/ or w/o hypoxia
CNS disease
Drug use (ASA, catechol, progesterone)
Pregnancy
Sepsis
Hepatic encephalopathy
Mechanical ventilation
Primary Respiratory Acidosis
eg. 7.25 / 60 / 80 / 26 = acute b/c no bicarbonate compensation
eg. 7.34 / 60 / 80 / 31 = chronic b/c bicarbonate compensation
CNS depression
Neuromuscular disorder
Acute airway obstruction
Severe pneumonia or pulm edema
Impaired lung motion (PTX)
Thoracic cage injury – flail chest
Ventilator dysfunction
Primary Metabolic Alkalosis (eg. 7.50 / 48 / 80 / 36)
* If Urine Cl is low: Vomiting, NG suction, diuretic use in past, post-hypercapnia
* If Urine Cl is normal-high: Excess mineralocorticoid activity, current diuretic use, excess alkali administration, refeeding alkalosis
Primary Metabolic Acidosis (7.20 / 21 / 80 / 8)
* Nonanion gap: GI bicarb loss (diarrhea, ureteral diversion), renal bicarb loss (RTA, early renal failure, carbonic anhydrase inhibitors, aldosterone inhibitors), HCl administration, post-hypocapnia
* Anion Gap: MUDPILES
Pearl: If anion gap>20 exists, there is a primary metabolic acidosis.
Pearl: If anion gap exists, calculate the excess anion gap to determine if an underlying metabolic alkalosis or nongap metabolic acidosis exists.
Examples
7.4 / 40 / 80 / 24, Na 145, Cl 100 --> Metab acidosis + metab alkalosis
7.5 / 20 / 80 / 15, Na 145, Cl 100 --> Resp alkalosis+ metab acidosis+ metab alkalosis
7.1 / 50 / 80 / 15, Na 145, Cl 100 --> Resp acidosis+ metab acidosis+ metab alkalosis
7.15 / 15 / 80 / 5, Na 140, Cl 110 --> Metab acidosis gap AND nongap